Projects Overview
Working with partners from multilateral institutions (including WHO, WHO/AFRO, and UNICEF) and leading disease-specific technical, policy, research, advocacy, and financing organizations, the NCDI Poverty Network co-secretariat based at the Center for Integration Science and Universidade Eduardo Mondlane in Mozambique supports national NCDI Poverty Commissions and Ministries of Health in lower-income countries through the four-stage process that leads from priority-setting through design and initial implementation to national scale-up of integrated service delivery models to address severe conditions affecting the world’s poorest children and young adults.
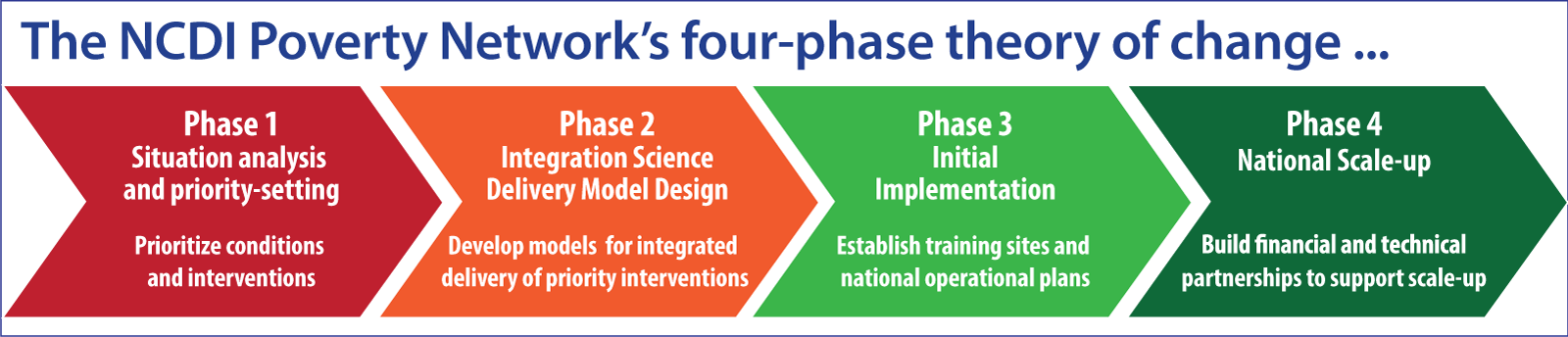
The Network Co-Secretariat delivers support through projects in six main areas:
- Equity-Driven Priority Setting – supporting countries that recently joined the Network and are conducting Phase 1 activities to identify priority conditions and interventions
- Task-Mapping and Delivery Model Design – supporting countries that are engaged in Phase 2 activities with developing models for integrated delivery of priority interventions
- Service Delivery Implementation Support – providing technical, policy, and administrative support to countries that are initiating implementation (Phase 3) of the PEN-Plus model for decentralization and integration of chronic care services for severe NCDs at first-level hospitals
- Curriculum and Training Material Development – supporting Phase 3 countries with establishing training and mentorship programs for mid-level providers to lead PEN-Plus clinics
- Evaluation and Impact Assessment – supporting M&E and research in Phase 3 countries to evaluate the implementation and impact of PEN-Plus services
- Advocacy and Communications – working with national commissions, partners across the NCDI Poverty Network and PEN-Plus Partnership, and all the CIS and Network Co-Secretariat teams to support activities across all four phases by raising awareness and mobilizing a global movement of solidarity to provide technical, policy, advocacy, and financing support
Equity-driven Priority Setting
Developing and Disseminating Equity-Driven Priorities and Policy Recommendations
The CIS Policy Team supports national NCDI Poverty Commissions with conducting equity-based situation analysis and priority-setting and producing reports to disseminate key findings and policy recommendations. Drawing on the experience of serving as the Secretariat for the Lancet NCDI Poverty Commission and supporting national NCDI Poverty Commissions, the team shares analytical frameworks, methods, and tools to support: assessment of the national burden of NCDs and injuries, disaggregated by age, sex, socioeconomic status, and geographic location; prioritization of conditions that disproportionately impact people living in extreme poverty at young ages; and prioritization of interventions based on equity (priority to the worse off in terms both of lifetime health and socioeconomic status), cost-effectiveness, and financial risk protection, with special attention to interventions that address prioritized conditions.
Priority-setting tool
The CIS research team is working in collaboration with the Bergen Center for Ethics and Priority Setting in Health at the University of Bergen (BCEPS) and the Disease Control Priorities project at the University of Washington (DCP), on development of FairChoices – a web-based decision-support tool for policy makers working on health benefit packages and universal health coverage priorities. The tool has been designed so that it can be tailored to national priority-setting processes and makes evidence on cost-effectiveness, equity impact, and financial risk protection more easily available to policy makers who have little technical background in these methods. The CIS team is responsible for incorporating analysis of condition severity as a dimension of equity and of integrated care teams to deliver packages of prioritized interventions.
Task-mapping and delivery model design
Facility assessment and task-mapping
The CIS Research team supports a subset of national NCDI Poverty Commissions that have completed the Phase 1 priority-setting process in conducting primary data collection aimed at documenting the current availability and organization of prioritized services, as well as developing recommendations on how to redesign services at different levels of the heath system for expanded access to care. The team has worked with partners to develop protocols and tools for rapid organizational assessments at the facility level to better characterize the delivery of specified high priority NCDI interventions.
Integrated service delivery model design
Building on work from Phase 1, in which national NCDI Poverty Commissions identify priority conditions and interventions, the CIS research team is working with partners, including a number national NCDI Poverty Commissions, to develop proposals aimed at service integration that optimizes workflows in order to overcome health system constraints, progressively decentralizes priority interventions, and improves access and quality of care at lower levels of the health system. In support of this effort, the team has adapted methods previously developed in high-income countries – such as task mapping and time-driven activity-based costing.
The team is working with partners in several countries to document the current organization of prioritized interventions in three clinical areas – acute care, chronic outpatient care, and advanced gynecologic and breast health – and estimating the costs and impact of redesigning existing services to package these interventions and deliver them through integrated care teams at first-level hospitals. Elsewhere, the CIS team and partners from the Bergen Center for Ethics and Priority Setting in Health (BCEPS) are working to analyze opportunities more broadly for improving access, efficiency, effectiveness, and quality of service delivery for prioritized NCD interventions.
Service delivery implementation support
The CIS Programs team leads support for implementing partners and Ministries of Health in countries initiating PEN-Plus programs and coordinates support from the Training Team for curriculum and training material development, the Research and M&E team for evaluation and impact assessment, and the Administrative team for program management, budgeting, and procurement. Programs team projects include:
Development of data systems for strong Monitoring & Evaluation
The foundation of effective monitoring, management, and evaluation of PEN-Plus implementation at facility, national, and multi-country levels rests on development of strong and compatible systems for collecting, aggregating, and analyzing data, using a set of commonly defined and understood terms and indicators. Drawing on clinical forms from countries that have successfully implemented PEN-Plus, as well as input and feedback from specialists in conditions treated at PEN-Plus clinics, the CIS Program and Research & ME teams have developed and shared two essential tools for data collection: a data dictionary and clinical forms designed to match protocols, support quality care, and deliver standardized indicators.
The data dictionary will serve to standardize language for monitoring clinical outcomes and measuring success, develop a comprehensive approach to clinical form design, and build a common, crowd-sourced, and peer-reviewed set of internationally endorsed PEN-Plus clinical indicators. It has been shared as a spreadsheet with separate tabs for data to be collected from all patients (i.e., general clinical information and socioeconomic data) and for each of the conditions treated at PEN-Plus clinics (e.g.,diabetes, cardiovascular, sickle cell, respiratory, liver disease). Clinical form templates for PEN-Plus conditions developed by the team are being adapted for use in some Phase 3 countries, while serving as references for implementing partners in other countries that are editing existing forms to include elements from the data dictionary. In addition to the clinical forms, the CIS team has also worked with implementing partners to develop country-specific forms for collecting socioeconomic data in each of the ten Phase 3 countries, adapted to reflect local conditions and indicators collected in existing surveys.
Developing and sharing technical materials and other documentation
To ensure that the PEN-Plus intervention is packaged in a collaborative, informed, and detailed way to support initiation and scale-up at country level and inform the broader policy and advocacy agenda with WHO AFRO, UNICEF, and other key partners, the CIS team has developed and shared documentation covering all aspects of program implementation. Topics covered include: Staffing; Training (including didactics and protocols for treatment of heart failure, diabetes, sickle cell disease, and five other severe conditions treated at PEN-Plus clinics); Medications, Labs, and Equipment; Care Pathways; Infrastructure; Data Systems; Evaluation; Reporting; National Operational Planning; and Integration Science.
Supporting procurement of essential medications, labs, and equipment
Drawing on experience in countries that have successfully implemented PEN-Plus and input from clinical experts engaged in the NCDI Poverty Network and PEN-Plus Partnership, the Programs team has developed and shared lists of the essential medications, point-of-care and laboratory equipment and consumables, and other materials needed to provide treatment for PEN-Plus conditions. In addition, the team shared an initial procurement plan for equipment, reviewed it with implementing partners in each of the PEN-Plus countries, and worked with the Center’s Administrative team to procure certain items centrally for countries where they could not reliably be acquired locally.
Evaluation & Impact Assessment
Working with Ministries of Health, implementing partners, and other stakeholders in 10 countries that initiated PEN-Plus in 2022-23, the CIS Research and M&E team is leading a program of implementation science research to evaluate the effectiveness and cost-effectiveness of PEN-Plus, assess the acceptability and appropriateness of services, and understand the unique challenges associated with initiating the PEN-Plus model in new countries and scaling it up nationally. The team has developed the protocol for a mixed-methods evaluation of PEN-Plus initiation and implementation over a period of three years across 18 sites in ten countries. The evaluation will seek to understand outcomes in clinical implementation, training, and policy development, using data collected through a mix of quantitative surveys, routine reporting, routine clinical data, and qualitative interviews.
The team has mapped out a program of research and evaluation to be carried out over the three years that includes baseline, midline, and endline assessments; quarterly evaluations of clinical outcomes and training indicators; semi-annual qualitative formative assessments; and ongoing cost analysis and monitoring of MoH activities. To date, the team has developed questionnaires and supported the ten Phase 3 countries in conducting baseline assessments of the availability and organization of services for severe NCDs, including staffing; infrastructure; availability of essential medications, labs, diagnostics, and equipment; staffing; and health information and data systems. These baseline assessments will be followed by midline and endline assessments conducted in 2023 and 2024. In addition, the team has undertaken an initial series of qualitative interviews with key stakeholders in ministries of health in the ten countries, which will be followed up with a second set of interviews in the third year in order to understand the readiness and evolution of the policy environment around PEN-Plus.
Curriculum and training material development
A working library of training materials
Building on content gathered from 29 organizations, the Training Team has developed and shared 19 training slide decks and clinical protocols for management and treatment of chronic conditions across 8 clinical areas – Cardiovascular; Diabetes; Sickle Cell Disease; Chronic Respiratory Disease; Liver Disease; Chronic Kidney Disease; Mental Health; Palliative Care. Version 1 of the materials is now available to implementing partners on a shared drive. And the training resources will be continuously improved and expanded through an iterative process based on countries’ needs and feedback.
Development and testing of an e-learning platform
The training team is also developing and piloting an e-learning platform for the core PEN-Plus conditions. The e-learning platform has been designed to be responsive to country needs and complementary to other PEN-Plus training and programmatic materials. Training modules for heart failure and cardiovascular disease have been completed and piloted, and diabetes modules are under development. Version 1 of the materials is now available to implementing partners on a shared drive. And the training resources will be continuously improved and expanded through an iterative process based on countries’ needs and feedback.
Technical, policy, and financial resource mobilization
The Center for Integration Science Advocacy and Communications teams work to raise awareness of the need to prioritize access to care for severe conditions that disproportionately affect the world’s poorest children and young adults, to amplify the voices of people living with these severe conditions, and to mobilize a global campaign of solidarity to address these conditions as both a moral imperative and a key to achieving universal health coverage.
Voices of NCDI Poverty Advocacy Fellowship
The Voices of NCDI Poverty Advocacy Fellowship provides those with lived experienced with NCDIs in the countries representing the poorest billion with mentorship, training in building successful advocacy campaigns, financial compensation, and the opportunity to take a voting role in the governance of the NCDI Poverty Network. Fellows work closely with the Secretariat to develop annual work plans focused on building a community of people living with NCDIs, as well as amplifying and leveraging the experiences of Voices of NCDI Poverty advocates to build policy and fundraising support for the PEN-Plus Partnership.
Voices of NCDI Poverty Videos
The Voices of NCDI Poverty Videos project is a platform that shares stories and experiences of people living with NCDs and injuries in settings of extreme poverty, amplifying their voices to advocate for their own priorities and have a larger role in shaping national, regional, and global NCDI policies and programs. Since the project was launched in 2017, it has filmed, produced, and disseminated narratives with more than 30 people living with severe NCDIs, and has produced thematic, multi-country videos spotlighting severe conditions that disproportionately impact, including type 1 diabetes, rheumatic heart disease, and childhood and women’s cancers.
Mobilizing a Global Movement of Solidarity
The CIS Advocacy team engages with global and regional technical, policy, and financing institutions and with disease-specific NCD organizations to raise awareness of the impact of PEN-Plus, encourage other organizations and stakeholders to join the movement, and pursue global financing opportunities for further expansion of PEN-Plus implementation across countries within the NCDI Poverty Network.