Research
Informing the design, implementation, evaluation, and scale-up of integrated service delivery models
The Center for Integration Science research team works with partners and collaborators in lower-income countries and in regional and global institutions in applying integration science to inform the design, implementation, evaluation, and scale-up of models for decentralizing services progressively and integrating those services to optimize both health system resources and patient outcomes and well-being.
As part of this work, a special emphasis is placed on research, monitoring and evaluation of PEN-Plus activities. The research team also works with implementing partners to develop the logic model, theory of change, process and outcomes indicators, and systems for monitoring and evaluation of PEN-Plus and other integrated service delivery models.
The multidisciplinary research team includes clinical and public health researchers with expertise in disease progression, epidemiology, systematic reviews, health economics and health systems. Our work leverages both quantitative and qualitative tools to better understand the potential and realized impact associated with delivering best possible care for type 1 diabetes, operationalizing PEN-Plus, as well as the implementation challenges faced by diverse teams. Lessons learned from the development of this model are also being applied to an ever-growing number of clinical areas, with teams now poised to assess opportunities to strengthen existing pathways across a number of health systems.
Research by Center faculty, staff, and collaborating partners supports national commissions, ministries of health, and implementing partners in lower-income with conducting the analysis and developing the evidence base to work through the NCDI Poverty Network’s four-phase theory of change:
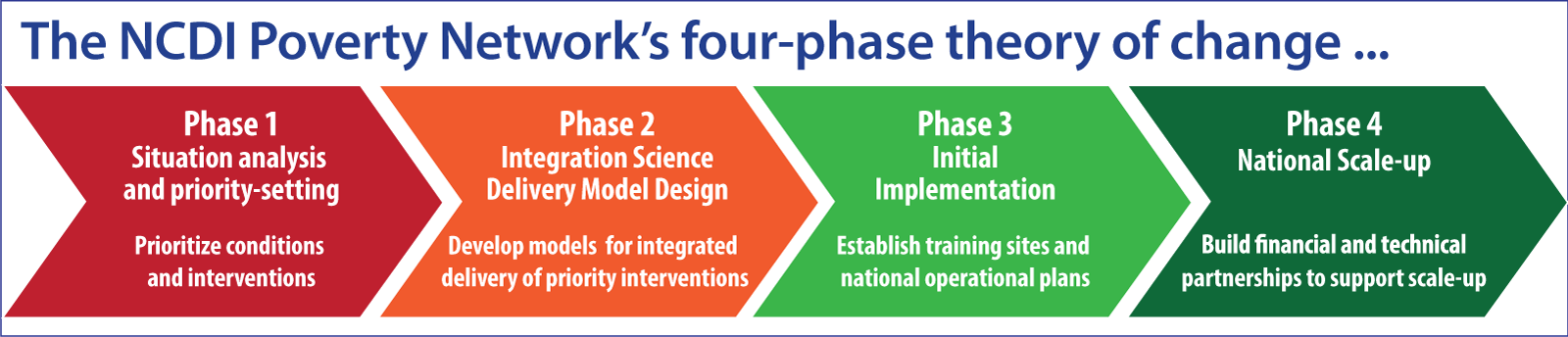
Situation analysis and priority-setting
The research team has worked to document the current and anticipated prioritization of severe, chronic NCDs, particularly across the WHO Africa region. A detailed review of national NCD strategic plans from across Sub-Saharan Africa documented a complex burden of disease, including simple and severe illness driven by a diverse array of risk factors. The policy response stood in stark contrast to this reality, frequently focusing on primary care targeting a small number of conditions.
In a separate survey of NCD technical leads across the region, we document that health ministries in Africa have ambitious plans to address gaps in availability of services for severe NCDs at lower levels of the health system by introducing and decentralizing care – particularly for conditions targeted by PEN-Plus. Additional work has focused on documenting the Commission process and resulting priorities.
Delivery model design
Work on delivery model design focuses on the clinical space, documenting the diversity of existing care models for individual conditions, assessing the readiness to provide priority care, and better understanding the current of clinical services across a range of settings. For individual interventions, this work focuses on understanding the nuances of care delivery – who delivers care, using what resources, and at what cost. In combination, this work forms the bedrock for work to design new, integrated delivery models aiming for UHC. With the use of modeling, we seek to quantify the potential impact of these recommendations.
Implementation, evaluation, and impact assessment
Much of our work is focused on understanding best quality of care based on both clinical indicators and patient experience. This falls into three categories: 1) determining best practices for T1D care in rural low resource settings; 2) implementation science; and 3) understanding implementation effectiveness and outcomes.
Examples of studies in best practice involve testing how programs that have been shown to be effective in high-income countries (for example diabetes self-management education and continuous glucose monitoring) can be modified for use in low-income settings. Implementation science research involves understanding barriers and facilitators to successful implementation. This includes evaluating the effectiveness and cost-effectiveness of PEN-Plus, and qualitative research around acceptability and appropriateness of services. Examples of studies around effectiveness include disease-specific cohort studies from three rural districts in Rwanda 10-year studies of the etiology of heart failure and outcomes of heart failure over a 10-year period, outcomes for RHD patients after cardiac surgery, and the effectiveness of the training model in Malawi.
Expansion and national scale-up of PEN-Plus
As we continue to expand PEN-Plus to an increasing number of countries and settings, it is important to understand the unique implementation challenges associated with initiating the model in new countries and scaling it up nationally in countries where it has been implemented successfully. This includes research around national scale-up in Rwanda and ongoing work in evaluating PEN-Plus expansion to ten countries (forthcoming).